ISSN: 2165-7904
Journal of Obesity & Weight Loss Therapy
������ý Access
Our Group organises 3000+ Global Events every year across USA, Europe & Asia with support from 1000 more scientific Societies and Publishes 700+ ������ý Access Journals which contains over 50000 eminent personalities, reputed scientists as editorial board members.
������ý Access Journals gaining more Readers and Citations
700 Journals and 15,000,000 Readers Each Journal is getting 25,000+ Readers
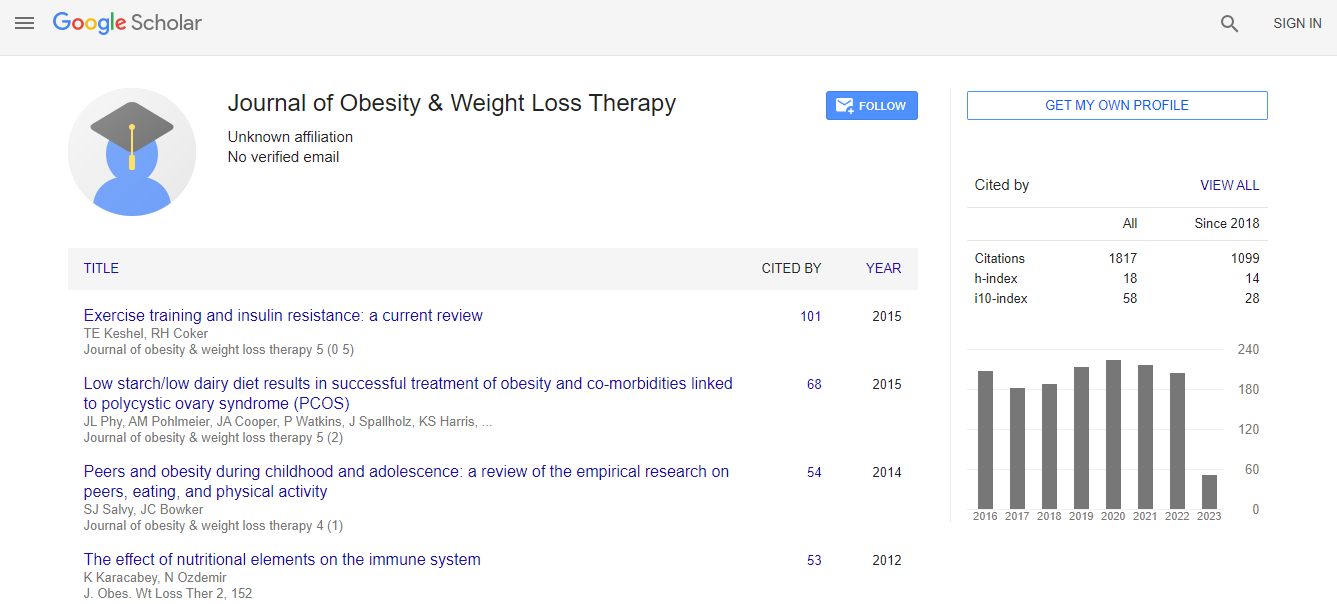
Citations : 2305
Indexed In
- Index Copernicus
- Google Scholar
- ������ý J Gate
- Genamics JournalSeek
- Centre for Agriculture and Biosciences International (CABI)
- RefSeek
- Hamdard University
- EBSCO A-Z
- OCLC- WorldCat
- SWB online catalog
- CABI full text
- Cab direct
- Publons
- Geneva Foundation for Medical Education and Research
- Euro Pub
- University of Bristol
- Pubmed
- ICMJE
Useful Links
Recommended Journals
Related Subjects
Share This Page
Contribution of prepregnancy weight and gestational weight gain to adverse pregnancy outcomes in Canada
6th World Congress on Obesity
Susie Dzakpasu
Public Health Agency of Canada, Canada
Posters & Accepted Abstracts: J Obes Weight Loss Ther
DOI: